Chest pain and related symptoms are one of the most common reasons for emergency department (ED) visits; however, less than 20% of these patients are eventually diagnosed with acute myocardial infarction (AMI).
High-sensitivity cardiac troponin (hs-cTn) assays are a key tool for diagnosis and exclusion of AMI, leading to improved patient outcomes. Timely diagnosis of AMI enables early treatment and decreases mortality. Moreover, faster triage of ED patients with suspected AMI can reduce ED overcrowding as well as reduce the risks of prolonged hospitalisation.
The ESC rapid ‘rule-in’ and ‘rule-out’ algorithms
The European Society of Cardiology (ESC) algorithms for rapid ‘rule-in’ and ‘rule-out’ of AMI is used by several institutions globally. The ESC 0/3-hour algorithm uses a cardiac troponin threshold based on the 99th percentile of a normal reference population at presentation and at the 3-hour mark, in conjunction with clinical criteria, to rule out or rule in AMI. Whereas the ESC 0/1-hour and 0/2-hour algorithms triage patients using hs-cTn thresholds lower than the 99th percentile of a normal reference population at presentation along with absolute changes within the first or second hour. It should be noted that all 3 algorithms are to be used in conjunction with a detailed clinical assessment that includes focused history taking, electrocardiography, and adjunctive imaging.
The ESC 2020 guidelines recommend 0/1-hour and 0/2-hour algorithms as the first and second choices while the 0/3-hour algorithm is recommended as an alternative to the other algorithms. The modest sensitivity (90% to 95%) associated with the 0/3-hour algorithm is responsible for this recommendation.
Meta-analysis to evaluate the diagnostic accuracies of the ESC algorithms
An International Collaborative Meta-analysis, published in the Annals of Internal Medicine in 2022 evaluated the diagnostic accuracies and triage efficacies of the ESC 0/1-hour, 0/2-hour, and 0/3-hour algorithms.
How was the meta-analysis conducted?
The study analysed 32 studies (published between 1 January 2011 and 31 December 2020) with 20 cohorts including 30,066 patients to compare the three algorithms for adult patients presenting with suspected AMI. The authors gave special consideration to study- and population-level differences.
The studies were either randomised controlled trials, prospective cohort studies, or implementation studies that evaluated the diagnostic accuracy of the three algorithms in adult patients presenting to the ED or chest pain unit with suspected non-ST-elevation myocardial infarction (NSTEMI) or acute coronary syndrome. The diagnostic accuracies of the algorithms were measured in terms of the sensitivity, specificity, negative predictive value (NPV), and positive predictive values (PPV) with index admission AMI.
Key insights from the study
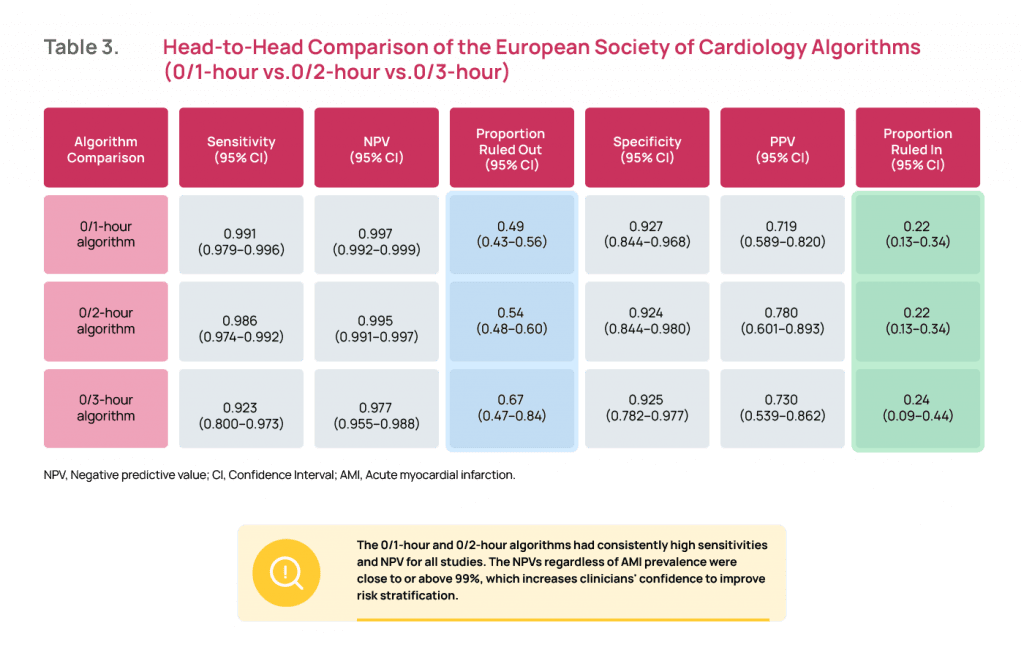
The ESC 0/1-hour and 0/2-hour algorithms showed higher sensitivities and NPV than the 0/3-hour algorithm for index AMI. Both algorithms had consistently high sensitivities and NPV across different population demographic characteristics.
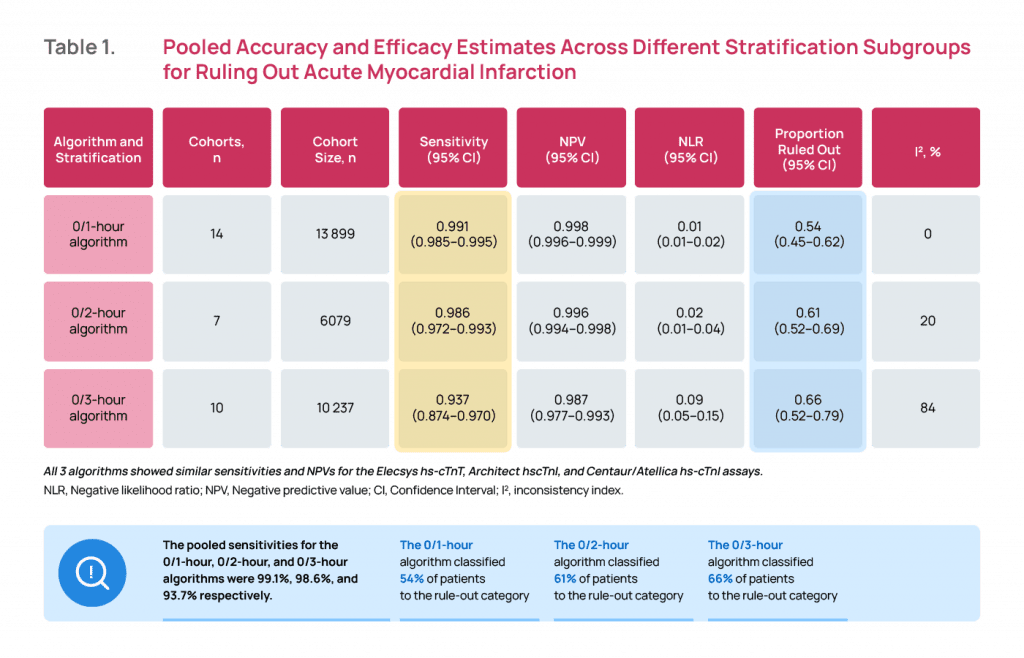
The 0/1-hour algorithm had a pooled sensitivity of 99.1% and NPV of 99.8% for ruling out AMI. The 0/2-hour algorithm had a pooled sensitivity of 98.6% and NPV of 99.6%. The NPVs for all studies, regardless of AMI prevalence, were close to or above 99%, which mirrors the safety estimates proposed by other investigators.
The 0/3-hour algorithm had a pooled sensitivity of 93.7% and NPV of 98.7%. Many studies reported an NPV of only 95% to 98% for the 0/3-hour algorithm, indicating a 2% to 5% miss rate for AMI.
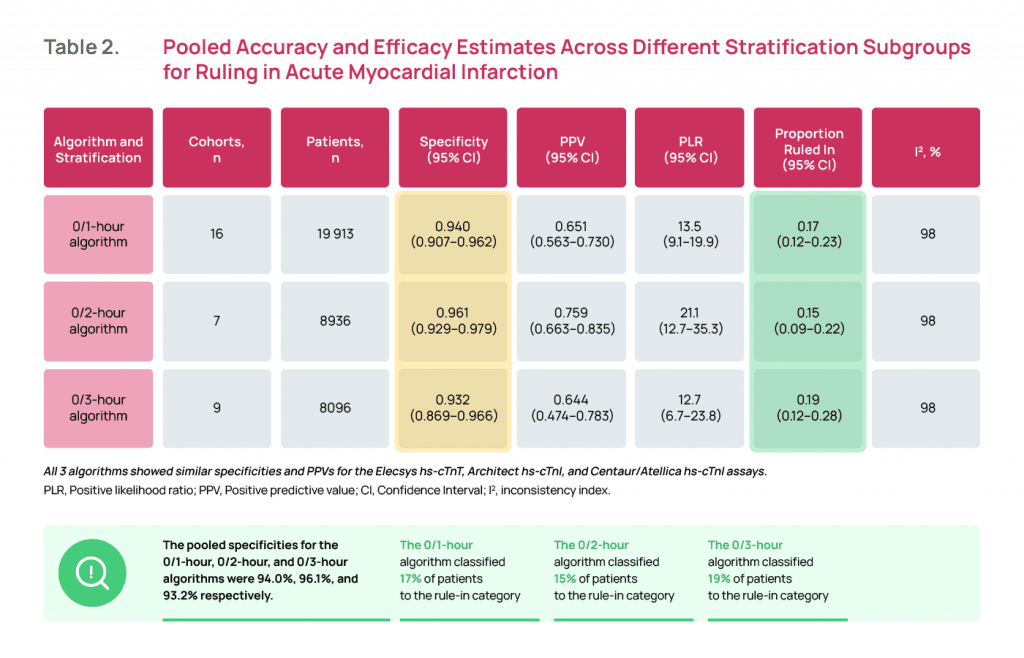
Diagnostic performance was found similar across the hs-cTnT (Elecsys; Roche), hs-cTnI (Architect; Abbott), and hs-cTnI (Centaur/Atellica; Siemens) assays.
Rapid Algorithms – What are the clinical implications?
Selecting the best triage algorithm is essential to improving patient outcomes. Emergency department physicians need high sensitivity to confidently rule-out AMI. On the other hand, cardiologists want to avoid false positives among patients identified as high risk in the ED.
Compared to the 0/3-hour algorithm, the ESC 0/1-hour algorithm has higher diagnostic accuracy, allowing safe rule-out as well as accurate rule-in of AMI. The 0/1-hour algorithm allows clinical decision-making two hours earlier compared with the 0/3-hour algorithm- this can reduce the total time to discharge, and treatment costs due to the considerable reduction in length of stay in the ED. Moreover, the 0/1-hour algorithm is more feasible as it does not require the use of a specific risk score.
The meta-analysis supports the changes reflected in the latest ESC guidelines and found strong evidence that the 0/1-hour algorithm has high sensitivity and NPV for index AMI. 0/1-hour and 0/2-hour algorithms use a much lower threshold of cardiac troponin concentration to rule out AMI at presentation and a low delta change between the first and second sample, which had been shown to have very good safety. The 99th percentile threshold used in the ESC 0/3- hour algorithm may result in a considerably high number of false-negative results.
The rapid algorithms can be implemented across populations with different demographic characteristics; however, the algorithm needs to be validated in regions such as South Asia, the Middle East, and Africa. Additionally, further studies are required to validate these algorithms in high-risk subgroups, such as patients with renal failure undergoing hemodialysis.

















