

In China, the number of dialysis patients is on the rise, and the incidence of heart failure in dialysis patients has remained high.
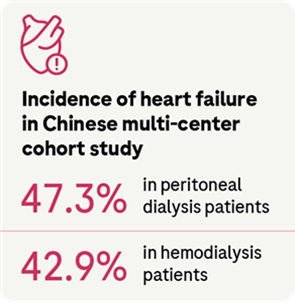
It is estimated that the number of dialysis patients in China will exceed 870,000 in 2025. A multi-center cohort study of 2388 Chinese dialysis patients (1775 on hemodialysis and 613 on peritoneal dialysis) found that the incidence of heart failure was 47.3% in peritoneal dialysis patients and 42.9% in hemodialysis patients.
Since dialysis patients have almost no residual renal function and many chronic complications, combined with the particularity, variability and limitations of hemodialysis and peritoneal dialysis, it is particularly important to protect the cardiac function of dialysis patients.
The diagnosis, treatment, and management of risk factors differ significantly between dialysis patients and the general population.
Heart failure is the second most common cardiovascular disease in dialysis patients. Once dialysis patients are complicated with heart failure, the survival rate is significantly reduced. Based on medical evidence and clinical experience, the Chinese Medical Association Nephrology Branch and the Zhongguancun Nephrology & Blood Purification Innovation Alliance Working Group jointly drafted the first “Guidelines for the management of chronic heart failure in dialysis patients in China”, in order to standardize the clinical management process of heart failure in dialysis patients and improve patient outcomes.

1. Diagnosis of heart failure
The diagnosis and evaluation of heart failure depends on history, physical examination, laboratory tests, cardiac imaging, and functional tests.
Table 1. Diagnostic criteria for heart failure
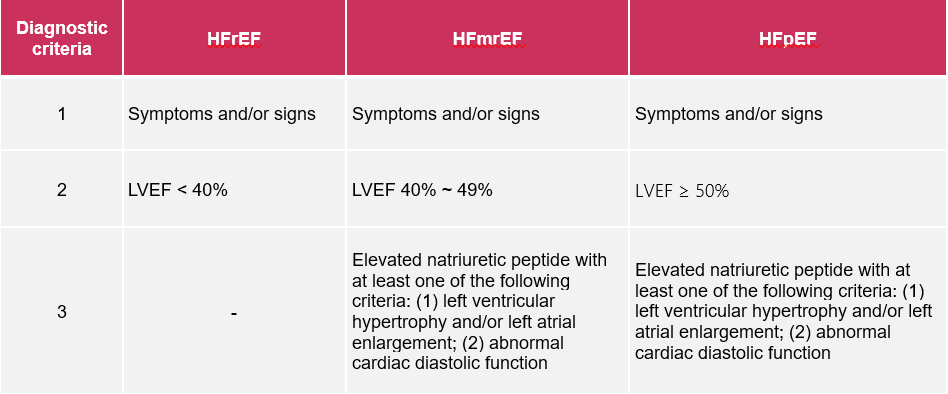
Note: HFrEF: heart failure with reduced ejection fraction, research status on it: randomized clinical trials mainly include such patients, and effective treatment has been proven; HFmrEF: heart failure with median ejection fraction, research status on it: the clinical characteristics, pathophysiology, treatment and prognosis of these patients are still unclear, and the single listing of this group is conducive to relevant studies; HFpEF: heart failure with preserved ejection fraction, research status on it: the patient’s symptoms need to be ruled out as being caused by a non-cardiac condition, and effective treatment has not been established; LVEF: left ventricular ejection fraction; elevated natriuretic peptide as B-type natriuretic peptide (BNP) > 35 ng/L and/or N-terminal B-type natriuretic peptide (NT-proBNP) > 125 ng/L; indicators of abnormal diastolic function are shown in the transthoracic echocardiography in the diagnosis and evaluation of heart failure.
a. Symptoms and signs
Main symptoms: dyspnea, fatigue, and fluid retention.
Characteristic signs include moist rale, peripheral edema, jugular vein engorgement, hepatojugular reflux sign, changes in apical pulsatile position, third heart sound gallop and heart murmur.
It should be noted that since the above symptoms and signs can also be seen in dialysis patients with volume overload, it is clinically difficult to distinguish heart failure from systemic volume overload. As a result, early heart failure symptoms in dialysis patients are often ignored.

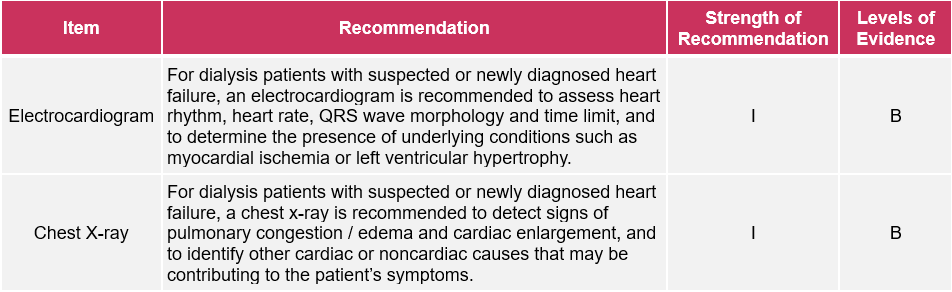
b. Routine examinations
Routine laboratory tests, ECG, chest X-ray, biomarkers, and echocardiography, etc.
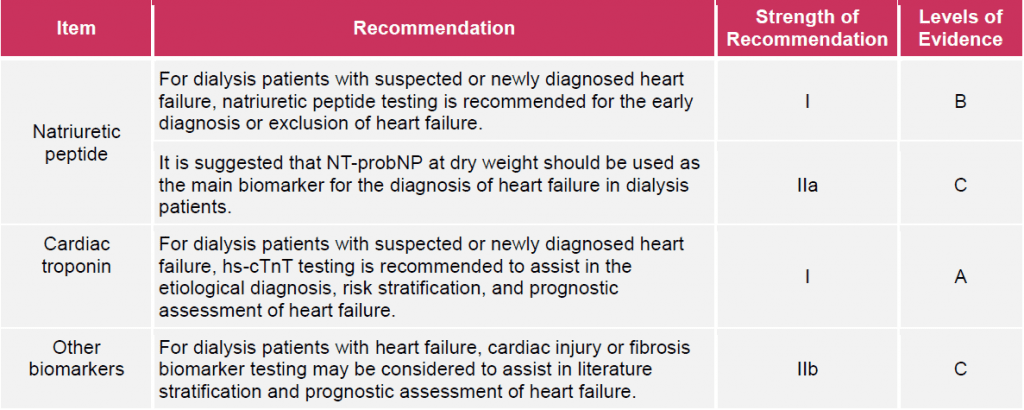
2. Biomarker
a. Natriuretic peptide (NT-proBNP or BNP)
In dialysis patients, elevated BNP levels can still reflect the presence and severity of heart failure and provide prognostic information, but the diagnostic cutoff value should be adjusted according to renal function. The available research evidence suggests that:
- NT-proBNP is more predictive of heart failure than BNP;
- It is suggested to use NT-proBNP as an indicator for evaluating heart failure in dialysis patients: the half-life of NT-proBNP (60-90 min) is longer than that of BNP (20 min), and the concentration of the former in plasma is also higher than the latter, which is more convenient for clinical detection;
- Existing clinical studies have shown that the optimal cutoff value of NT-proBNP for the diagnosis of heart failure in ESRD patients is 11215.2 ng/L; however, the accuracy and validity of this criterion still need to be confirmed in independent prospective studies and clinical practice.
b. Cardiac troponin (cTn)
Troponin T (TnT) has a higher predictive value for prognosis than troponin I (TnI), and hs-TnT is more widely used because its sensitivity is higher than that of TnT.
hs-TnT increases slightly with the progression of renal insufficiency, and the cutoff value for prognosis evaluation should be adjusted according to renal function: studies have shown that the optimal cutoff value of hs-TnT for predicting all-cause mortality in patients with CKD Stage 4 to 5 is 40 ng/L.
c. Echocardiography
Echocardiography is an important examination in the diagnosis of heart failure, and is also the first choice to evaluate the cardiac structure and function. In dialysis patients, echocardiographic indicators that should be of particular concern include left ventricular size and wall thickness (to assess the presence of left ventricular hypertrophy and geometry), LVEF, left ventricular diastolic function, valve appearance and function, left atrial pressure, and pulmonary artery systolic pressure.

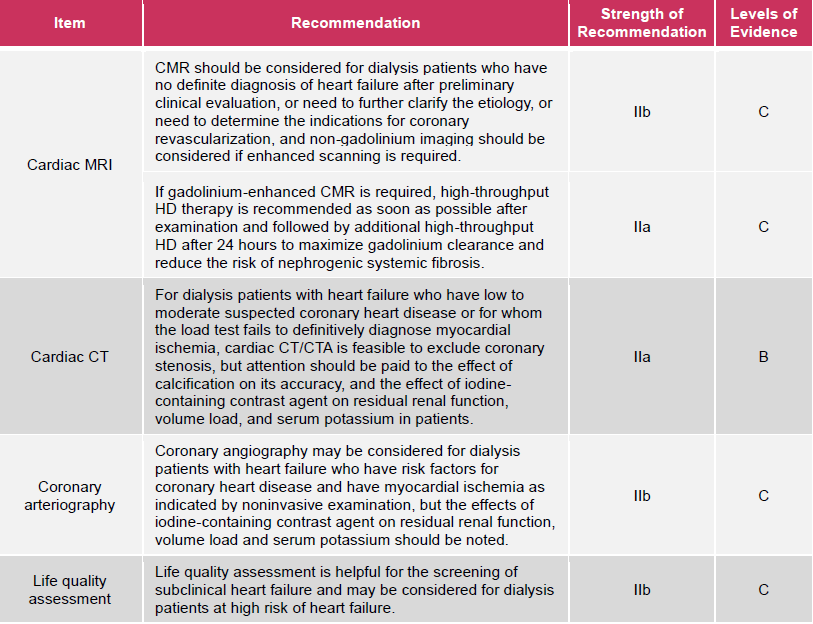
3. Special examination
Special examinations for heart failure are suitable for patients who need to further clarify the etiology and condition evaluation, mainly including cardiac MRl, cardiac CT, coronary angiography, and quality of life assessment.

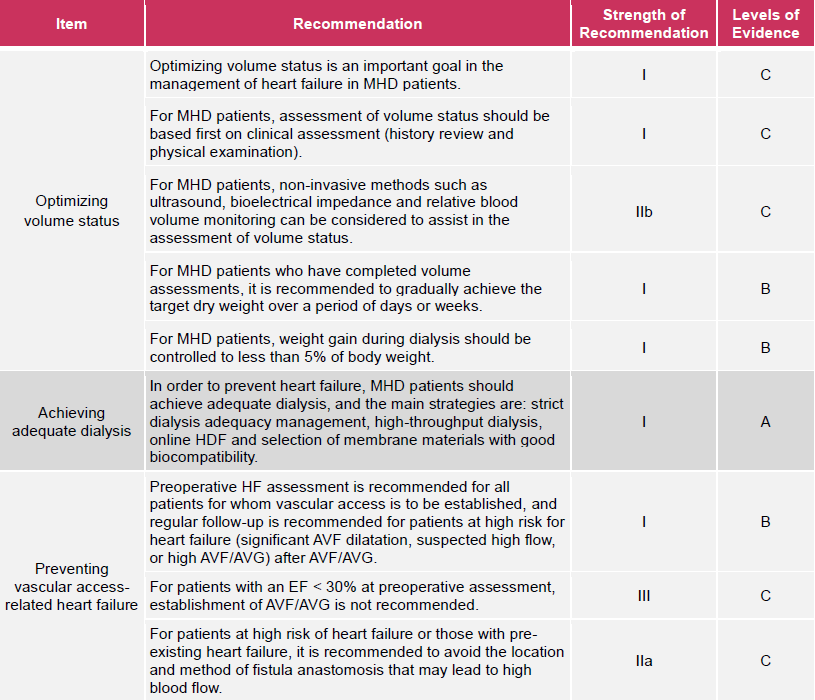
4. Heart failure management in dialysis patients
Hemodialysis management: prevention of heart failure in maintenance hemodialysis (MHD) patients.
The prevention of heart failure in MHD patients mainly includes optimizing volume status, achieving adequate dialysis, and preventing vascular access-related heart failure.
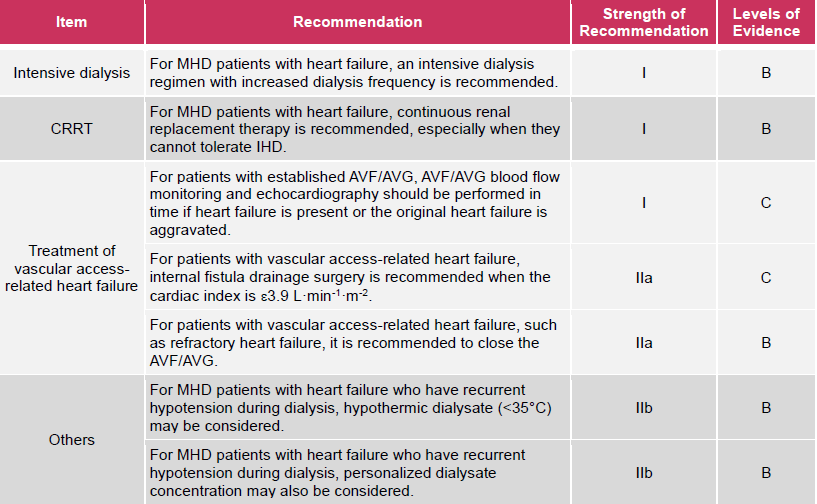
Treatment of heart failure in MHD patients
Intensive dialysis, continuous renal replacement therapy (CRRT), and treatment of vascular access-related heart failure are important aspects of hemodialysis treatment in MHD patients with heart failure.
Peritoneal dialysis (PD) management
PD is a home-based therapy that continuously removes sodium and water to maintain good volume status and avoids the risk of heart failure associated with vascular access, so it is considered an appropriate treatment for dialysis patients with heart failure, especially those with refractory heart failure.

Prevention of heart failure in PD patients
The prevention of heart failure in PD patients mainly includes the optimization of non-drug therapy and PD prescription.
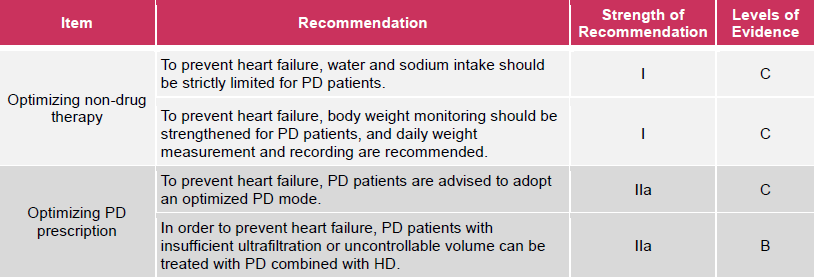
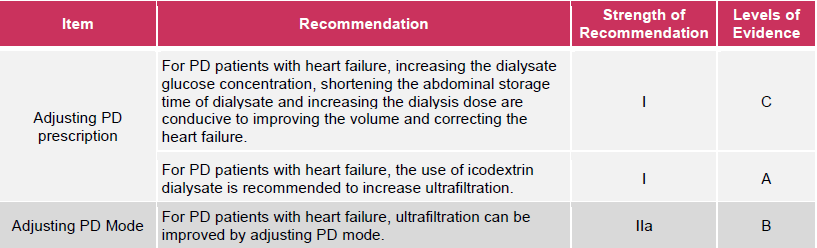
Treatment of heart failure in PD patients
The treatment of heart failure in PD patients mainly includes adjustment of PD prescription and PD mode.

5. Drug management
Drug management therapy remains an integral part of the treatment of dialysis patients with heart failure. Experts have formed preliminary consensus opinions on drug therapy based on the limited clinical evidence available, but these opinions still need to be further refined in clinical practice.
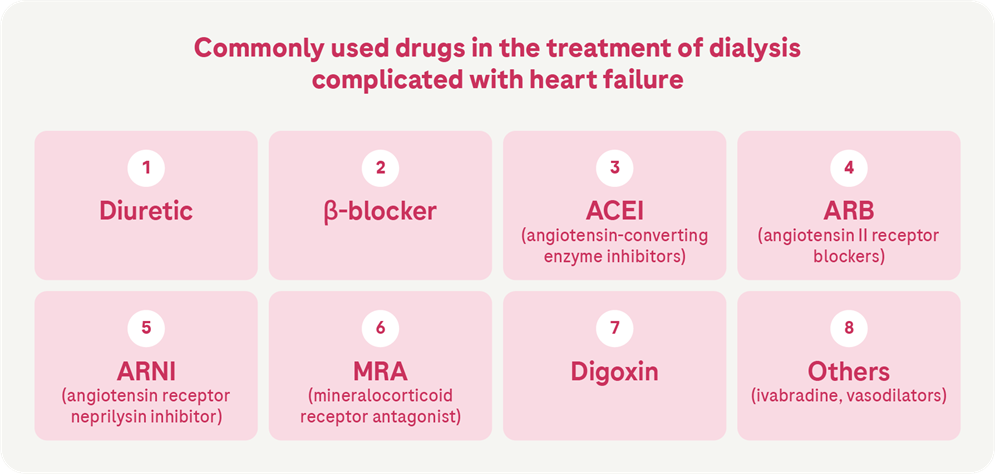
Commonly used drugs in the treatment of dialysis complicated with heart failure are diuretics, β-blockers, angiotensin-converting enzyme inhibitors (ACEI), angiotensin II receptor blockers (ARB); angiotensin receptor neprilysin inhibitor (ARNI); mineralocorticoid receptor antagonist (MRA), digoxin and others.
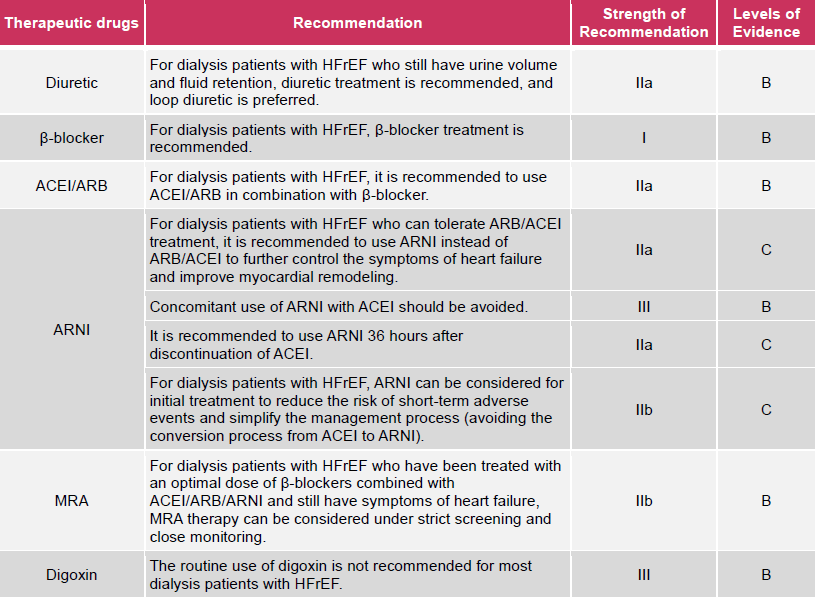
Dialysis with reduced ejection fraction
Drug management in patients with heart failure (HFrEF)
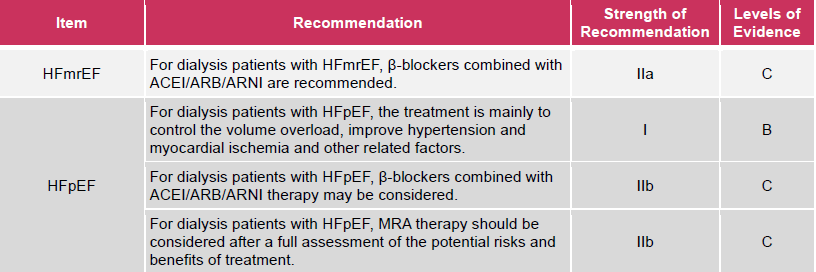
Drug management of dialysis patients with heart failure with mildly reduced ejection fraction (HFmrEF) and heart failure with preserved ejection fraction (HFpEF)
References:
Chinese Medical Association Nephrology Branch, Zhongguancun Nephrology & Blood Purification Innovation Alliance. Guidelines for the management of chronic heart failure in dialysis patients in China [J]. Chinese Journal of Nephrology, 2022, 38(5): 465-496. DOI: 10.3760/cma.j.cn441217-20210812-00068.

















